PA Practice Modernization
Patients deserve modern, integrated healthcare delivery led by healthcare providers who are all practicing to the top of their scope of practice.
Physician associates (PAs) are committed to making this a reality through PA practice modernization.
What is PA practice modernization?
The first PA practice laws were enacted by states in the 1970s and must be continually updated to keep pace with changes and innovations in healthcare delivery.
Modernizing PA practice laws unlocks the full potential of the PA profession and can help to ensure patients in all communities have access to timely, affordable, and high-quality care.
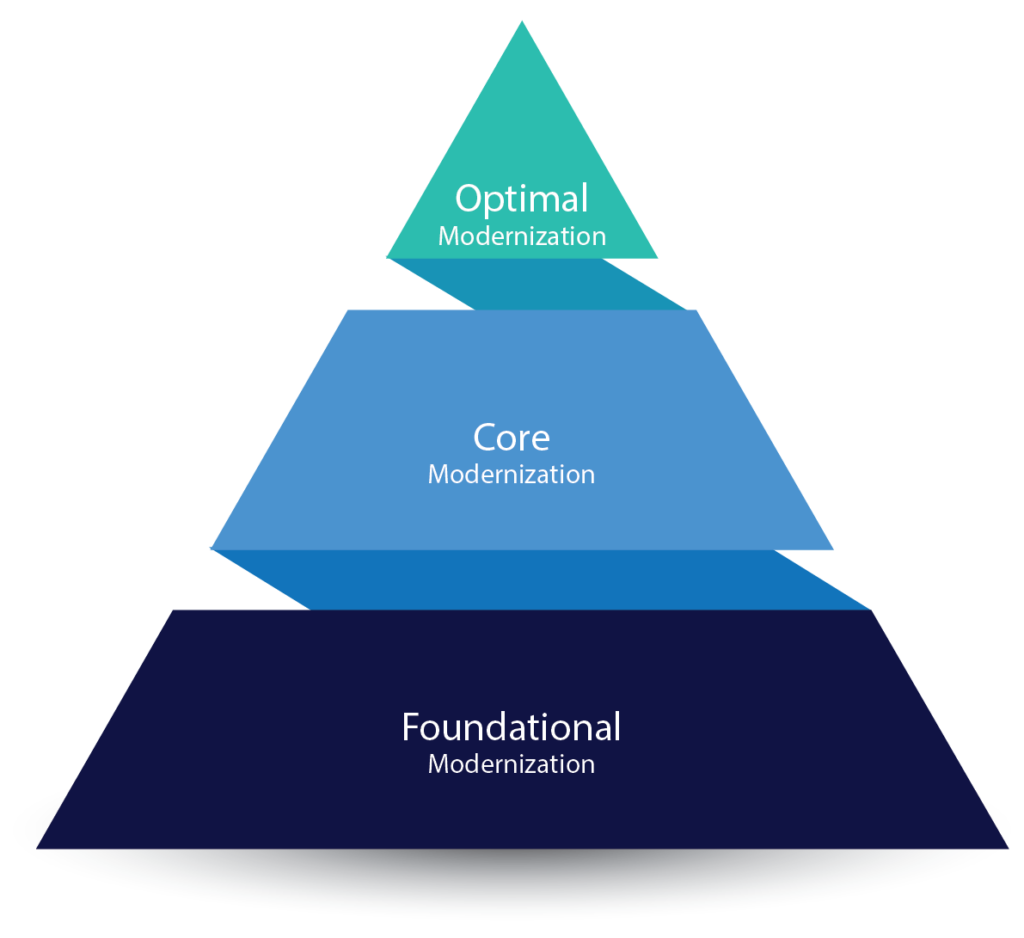
Optimal Modernization
- Removal of the legal tether between a PA and physician (such as a requirement for a written agreement)
- A separate PA regulatory board or one or more full PA voting member(s) on the medical/healing arts board
- Direct pay to PAs (as opposed to practice/employer)
Core Modernization Examples
- PA Licensure Compact
- Title Change
- Harmonization Acts
- Form Authentication (death certificates, handicap placards, POLST, MOLST, home health orders)
- Move from “supervision” to “collaboration”
- Scope of practice determined by PA’s education, training & experience
- PAs “practice medicine”
- PAs responsible for care provided
- Elimination of physician delegation
Foundational Modernization
- “Licensure” as the regulatory term
- Scope of practice determined at the practice level
- Full prescriptive authority
- Adaptable proximity
- Co-signature requirements determined at the practice level
- No restrictions on the ratio of PAs to MDs or DOs
Views on Practice Modernization
92%
of U.S. adults agree PAs should be utilized to address healthcare workforce shortages.
91%
agree PA practice laws should be updated to allow states and healthcare systems to fully utilize their healthcare workforce.
Practice Modernization in Action
How can PA practice modernization improve patient access to high-quality care? See the difference a 2023 law enacted in Iowa has made!

PA Practice Modernization FAQ
Read the FAQ below to learn more about PA Practice Modernization. Don’t see your question here? Email us!
One of the fastest-growing healthcare professions, PAs are essential to addressing healthcare access challenges in our country. PAs have more than 590 million interactions with patients each year. With modernized PA practice laws, the PA workforce could more effectively meet patient needs and play a greater role in efforts to address health disparities and close gaps widened by shortages in the healthcare workforce.
Patients agree.
A 2023 survey from The Harris Poll found that 92% of U.S. adults agree PAs should be utilized to address healthcare workforce shortages, and 91% agree PA practice laws should be updated to allow states and healthcare systems to fully utilize their healthcare workforce.
Ultimately, when state laws and regulations remove the legal requirement for PAs to have a specific relationship with a physician, patients will have greater access to care, especially for medically underserved populations and patients in rural areas.
By removing the legal tether requiring a PA to be supervised by a physician, healthcare employers have great flexibility in building their provider teams. When a PA isn’t required to have a specific relationship with a physician, their employer can be more flexible in creating healthcare teams, allowing them to more effectively meet patient needs and reduce provider burnout.
Ending this requirement also removes physician liability for the care that PAs provide when physicians are not involved and reduces physician and employer risk of disciplinary action for administrative reasons. Also, allowing PAs to receive payments directly will expand the number of available providers through the use of healthcare staffing companies and other business arrangements that require PAs to reassign insurance payments.
No. A PA’s scope of practice is based on their education, training, experience, and competency, and includes the professional activities they are qualified and authorized to perform.
AAPA advocates for the full removal of any legal requirement for a PA to be supervised by a specific provider and supports collaborative, team-based care that is determined at the practice level depending on a patient’s needs.
Healthcare delivery by collaboration is a model that prioritizes patients, not any one provider. Outdated laws requiring physician-led teams fail to account for the full spectrum of providers that are available to meet the unique needs of the patient and risk patient health outcomes with delay, lack of access, and higher cost of care. In some cases, when the supervision requirement or “legal tether” to a physician is removed, state laws and regulations may require a collaboration agreement between PAs and other providers. In that case, AAPA supports collaboration agreements that include not just physician collaboration, but also other providers as appropriate to meet the needs of the patient and as determined at the practice level (not by a prescriptive or limiting statutory or regulatory construct). The physician-led model is an outdated construct that no longer meets the needs of patients in modern healthcare systems and fails to recognize the ability of teams to be led by PAs or other providers.
Today, physicians are regulated by state medical boards composed of physicians. Nurses are regulated by boards made up of nurses. Only PAs are regulated by boards that often have no members actively working in their own profession. This means the boards that regulate PA practice may lack knowledge of current PA practice or how rules and regulations may affect PA practice. This dearth of insight can lead to unnecessary restrictions and administrative burdens for PAs, physicians, and employers.
PAs deserve what physicians and nurses already have: regulatory boards with current knowledge about their profession. States can determine whether this is best accomplished by creating separate PA boards or by adding PAs and physicians who work with PAs to medical or healing arts boards. Read more.
North Dakota, Utah, Wyoming, Iowa, New Hampshire, South Dakota, Oklahoma, and North Carolina have all enacted laws to remove the legal requirement for PAs to maintain a formal supervisory agreement with a physician.
These updates allow PAs to practice more autonomously (based on their training and licensure), expand access to care (especially in underserved areas), reduce administrative burdens, improve team flexibility, and reflect a growing national trend toward modernizing PA practice laws
In 2008, AAPA identified six foundational components that we believe all PA practice acts should contain.
Coined the “6 Key Elements of a Modern PA Practice Act,” many of these components continue to serve as the foundational beginnings for the creation of a more efficient PA practice environment while simultaneously protecting public health and safety.
The Six Key Elements established in 2008 were:
- “Licensure” as the regulatory term
- Full prescriptive authority
- Scope of practice determined at the practice level
- Adaptable proximity requirements
- Cosignature requirements determined at the practice level
- Number of PAs a physician may collaborate with determined at the practice level
Learn more: The Six Key Elements of a Modern PA Practice Act.
“Optimal Team Practice” (OTP) is a policy that was adopted by AAPA’s House of Delegates in May 2017. The twofold purpose of the policy is to:
(1) reinforce the profession’s commitment to team-based patient-centered practice, and
(2) relieve PAs, physicians, and employers from unnecessary burdens imposed by antiquated laws and regulations that pose needless delays in a patient’s ability to access healthcare.
To achieve these goals, the policy emphasizes the importance of amending statutes and regulations to authorize:
- Remove supervision requirement: PAs to practice to the full extent of their education, training and experience absent a mandated relationship to a specific healthcare provider
- Representation on regulatory boards: PAs to meaningfully participate in the regulation of the PA profession through the creation of a separate majority-PA board or the addition of PAs and physicians who work with PAs to medical or healing arts boards in which they will be full voting members of the board, and
- Direct pay: PAs to be eligible for direct payment by all public and private insurers
Learn More: PAs and Team Practice
The current legal requirement in nearly all states for a PA to have a specific relationship with a physician doesn’t align with current PA practice — or how healthcare is delivered to patients. “Specific relationship” represents a legal tether, which may come in the form of a practice agreement with a physician, or another type of arrangement, like the requirement for PAs to complete a form that designates a specific physician with whom they work. Regardless, any type of legal tether between a PA and another provider can be incredibly burdensome, not only for the provider but also for the health system or facility.
A legal tether to a physician can also limit where PAs can practice. Physician shortages across the country mean there are not enough physicians to supervise available PAs and limits employers’ ability to hire more PAs to address patient demand. The PA profession is growing seven times faster than physicians. A shortage of 55,000 US primary care physicians is anticipated by 2034. Removing the legal tether unlocks PAs’ ability to meet patient demand.
Thanks to advocacy work led by AAPA, Medicare has authorized direct payment to PAs since 2022, However, some insurers and even state laws limit payment to a PA’s employer. Direct payment is important. It allows a PA to receive payment for their services directly or reassign that payment to someone other than their employer. Without this payment option, it can unintentionally limit PA employment opportunities with staffing companies and in certain practice arrangements, such as when hospitals contract with a group practice to provide services.
As the healthcare system continues its rapid transformation toward more innovative care models, PAs must have the same reimbursement flexibility as other healthcare professionals so they can provide high-quality, cost-effective healthcare in a variety of settings and meet the needs of patients. Read more.
Today, physicians are regulated by state medical boards composed of physicians. Nurses are regulated by boards made up of nurses. Only PAs are regulated by boards that often have no members actively working in their own profession. This means the boards that regulate PA practice may lack knowledge of current PA practice or how rules and regulations may affect PA practice. This dearth of insight can lead to unnecessary restrictions and administrative burdens for PAs, physicians, and employers.
PAs deserve what physicians and nurses already have: regulatory boards with current knowledge about their profession. This is ideally achieved when states establish separate PA boards but at a minimum, regulatory boards must voting seats for PAs and physicians who work with PAs. Read more.